
Symptomatic care
Betadine Nasal Spray
Before the virus has finished moving through the linings of nose, sinuses, eustachian tubes of the ears, ...
let's kill it.
Let's kill it with betadine (povidone iodine).
Just another hairbrained idea from that guy in Belgium?

No, more than that source, there is some Science behind the idea.
In Vitro Efficacy of a Povidone-Iodine Nasal Antiseptic for Rapid Inactivation of SARS-CoV-2
one more ...
My experience in the past with Betadine (povidone iodine) was when we would paint a belly with it in preparation for an operation. And there, that was 10% povidone iodine.
Next door in another OR, an ENT surgeon was preparing to operate on a nose.
Noses are rather dirty inside from a bacterial/ viral standpoint.
It's why polite people sneeze into a hanky.
So the ENT surgeons would swab the inside of the nose with 5% povidone iodine before even thinking about making an incision.
Nice story. But so what today?
Well today, for Trish, let's get some povidone iodine spray into that nose that now has proven SARS-CoV-2 virus harbored within. Yuck. Yeww ...
Here's how.
Prior communications this day indicate familiarity with spraying saline in one's nose for good purpose. Even better, the presence of such material on hand.
She already has this ...

To start from scratch in this, doing it oneself, here's a little video, fresh off the camera.
Here is a link to the above video, if needed.
Mode d'emploi
Once you have this in hand, can think of it as either treatment, or prevention.
Prevention
Imagine you're in a setting with other people, not much ventilation, and no one is wearing a mask (except perhaps you).
Think of that still as rather a high risk of transmission setting.
This will of course vary with where you are located, which variants are around, etc.
Let's keep it simple.
So, when you get out of that setting, a spritz or two in each nostril, a good nose blow and a hand wash, and you may have just stopped a viral transmission from them to you.
Treatment
Now imagine that everything was just fine, and you started to feel something coming on.
Imagine you even have a test for the SARS-CoV-2 on hand. You take the test, and it's positive.
So now, you have COVID-19. That's an illness. If your test is positive but you have absolutely no symptoms, no loss of taste and smell, etc. Nothing, then that's the perfect situation in which doing the following may help keep you healthy. You don't have COVID-19 (illness); you are simply infected with the virus, and lucky so far because you don't feel sick.
Two spritzes in each nostril. Wait a bit. Blow your nose. Throw away the Kleenex. Wash or sanitize your hands.
Do this about every 8 hours for 3 to 5 days. Especially, after waking up, and before going to bed. (Which leaves a spritz session to be done at around noon).
For any questions, you have the email address.
An approach to "brain fog"
For those with the "long-term" variant of COVID-19, "brain fog" is a common complaint.
For them the nervous system was involved in 71%, second only to the respiratory system.
Again, the numbers come out of 136 respondents to my questionnaire, back in October.
In previous discussions, I have mentioned that the red light treatment has already been used with patients suffering Traumatic Brain Injury, improving their cognitive abilities.
An upcoming study (if I get it off the ground) will include focusing red light on the head.
Why target the head?
Because that's where many of their symptoms seem to be located. Here are the top 10
when symptoms are ordered by frequency.
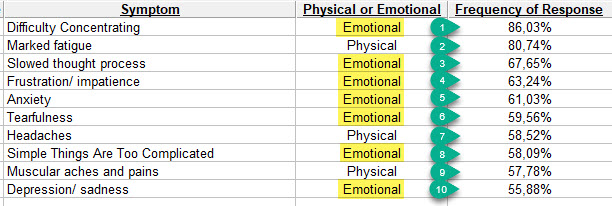
Of course, one need not have all of these. Let's come back to "brain fog." Not specifically on the list as such, but related to the top 3 or 4 that are.
Here is what I suggest. Do a little study!
Use the light that Trish has because it will be easier to manipulate. That, instead of manipulating one's head in front of the larger light.
We need a control to prove an improved effect (or none). Having other people involved as controls would be very professional, but not very practical.
Instead, let's use Lumosity to see if the "brain fog" clears a bit and scores improve over time or not. I think you have looked at Lumosity in the past. It just gets some people frustrated, but I think it's very well done, easy, and available.
The goal would not be to "prove one is the best." Instead, to see if using the light is associated with improving scores or not, over say a two week trial period.
I have a "Family Account" at Lumosity.
I will resend emails to set up participation.
Some neurologists would argue: this isn't virally induced "brain fog," it's just normal "old guy brain." What follows might help with that as well, if they're right. But I think that a virus-related brain effect is likely. More likely in those who started with GI symptoms than respiratory symptoms in fact, says the literature.
OK so what is the protocol?
First, a safety message. In all those treated with red light "helmets" so far, (this began 10 years ago), no side effects reported. No skin burns on top of the head. Shining a light on one's head instead of a knee may feel a little different at first, I'll grant you that. Takes a little getting used to, that's all. One can close one's eyes. Things will still look red behind closed eyelids. That should be Okay. Might even help.
- Do a Lumosity baseline test. Don't worry about the score obtained. It is what it is. It will serve to make comparisons.
- Using Trish's light held comfortably in hand, practice moving it before even turning it on. Here is the path, looking down on the head: I'll put these in an ordered gallery ...
The images show:
- the top of a head
- the right distance to hold the light away from the scalp (3.5 to 4 inches, being exactly always at the same distance doesn't matter in this experiment).
- the path to follow. Start behind the right ear. Move light forwards towards right eyebrow. Once arrived at mid-forehead, start backwards in middle of head until the bump back there on top is reached. Then move to left above and behind left ear. Work forwards towards left eyebrow. When you get there that's one "lap." Go back to behind right ear and start over.
- in subsequent images that path is numbered. At first count about one second per number: 1-2-3-4-5-6 (at mid-forehead) 7-8-9-10-11-12 (at bump towards back of head) 13-14-15-16-17-18 (near left eyebrow), and cross over and back to starting position.
- If one prefers, one can use the fixed larger light and move one's head. I think the smaller one held in hand is easier.
- How long? For about 6 minutes per treatment, 10 minutes max, divided between the 3 paths. It's good its not a longer duration or it would get very boring. Can continue to do the previous treatments to front and back with the larger light without discounting times or anything like that. 6 minutes on the head, not more than 10.
After 3 to 4 days of this, you may in fact begin to sense some improvement. You may be able to define this personally, better than Lumosity. If a mental jitteriness appears (different than anxiety or panic) take a day off.
I'd still use Lumosity each day or every other day for a week or two. Before or after a light session shouldn't matter. But that will provide some numbers, slightly more objective than an impression.
Now if this is actually "old person's brain" and not COVID-related "brain fog," who cares if some improvement comes out of all of this?
I'll send this note in a link, and send an invitation to Lumosity in case you don't still have your account. (I think they had told me that you already have an account). Let me know.
No pressure to do this. You decide.
Trish could do it too and serve as your control.
If you're both doing it, or Pete gets involved, one person could hold the lamp and do the other person's treatment. Might be easier to keep the desired distance from the scalp.
Kind of like going to the barber.
What else could you possibly want to be doing during a pandemic?
About that runny nose.
I copy Trish's last email in case you 3 haven't talked about this.
"I feel pretty good. I get a headache each afternoon and go to bed very early. I am such a night owl ordinarily. A bit of a drip from my nostrils occasionally. Not normal for me.
I am walking back and forth, over and over , on the balcony now. 1:45 today. Over 2 hours yesterday. Not all at once. A stroll, rather than at a real pace, but I keep at it. And so it goes!"
-------
I have highlighted the part I'll address in this little note.
A drip from the nose is called "coryza" in medical parlance.
Typically caused by inflammation of the nasal lining, most commonly observed with hay fever.
Almost an aside ...
Human, beings have about 40,000 or so thoughts per day.
Most of these never reached consciousness (so stay in the unconscious).
88% or so of these are negative thoughts ("Oh no! Not that I hope!" - or equivalent.
That is because negative thoughts contribute to our survival since millenia ...
"I hope that leaf moving in the jungle on my path just in front of me, doesn't have a tiger behind it. Gee. I'd better turn around or just stay put until the leaf stops moving."
So starting to talk about a drippy nose right away brings negative thoughts into my medically over-trained brain:
"Gee, I like Trish. I hope she doesn't have a runny nose that indicates a cerebrospinal fluid (CSF) leak due to:
-
-
- a brain tumor (always finds a place quickly on any list of the over-trained)
- damage to the blood-brain barrier when they stuck a long-Q-tip in her nose a few days ago and traumatized things.
- Churg-Strauss Syndrome (don't even bother looking it up)
- allergy
- a symptom of an infection by the SARS-CoV-2 virus, and now she has this as the only (rather less than common symptom, just as diarrhea is less than most common)
- acute sinusitis
- decongestant hasal spray overuse
- I'll stop there ...
-
So all of these are pretty rare causes of a drippy nose. I will skip the part which starts: "if its this, do this to prove it, and here is the treatment." Some, like Churg-Strauss Syndrome have no treatment. Swell. Already back into negative thoughts.
So what should be done?
-
-
- Accept that maybe it is COVID-19 presenting with some delay.
- We have already discussed that the reception to re-testing for the virus is not well received on this day by those who are in power where you are currently located. So probably, this close to the end of being quarantined, no go on obtaining that test. After this number of days, it would probably be negative and serve no purpose.
- BUT ... keep in mind that IF you do have it (but probably not given the entire history of events so far), an antibody test might be of use. Even if you felt fine when that blood test was done, a result that showed an increases level of antibody in the blood would permit someone to say: "Hey. You know what? You had COVID-19." (Assumes you haven't been vaccinated, of course).
-
So when it becomes possible to have a blood test for whatever reason that the medical establishment accepts, make an argument with those ordering tests, for getting a serum antibody level for the SARS-CoV-2 virus. Mike and Pete should also get one the next time that becomes feasible, but for different reasons in each of their two cases.
And that's it in the drippy nose department.
An additional observation.
Walking around your balcony for two hours every day, is quite understandable given everything related to your current imprisonment. Pardon me, I meant confinement in relatively comfortable circumstances. (More comfortable for instance, than a refugee camp in Syria).
But if outside of the present circumstances, an appropriate assessment by an overly-trained medical person might be: "OK. That's called physical perseveration, and a perfect example of an obesessive-compusive disorder aimed at minimizing an unrecognized fear carried in the unconscious ..." (or equivalent verbage). I'm not suggesting that diagnosis, since in current quarantined circumstances, that terrace walk seems perfectly defensible and what I would be doing if trapped in your shoes.
Here's another way to pass the time. It's even good for your head.
Perhaps you already do this. If so, let me know.
It's called Lumosity.
I purchased this as A Friends & Family Plan that renews in a year and did not
bankrupt me as Christmas presents go, so I'm grateful.
You will receive an email from Lumosity telling that you have each been gifted this.
In doing this I learned that Mike already has a Lumosity account (A Russian hacker confirmed that for me), so tell him to get on the stick and use his account. I'm betting on you Trish to beat his scores.
This may cut down on the walking in circles or rectangles on the terrace.
Just a few more days to go in quarantine.
Hell. I could do that standing on my head.
OK, gotta go. Still haven't unpacked my suitace from the planned Antarctica trip.
Damn.
Bill/ Uncle Billy
Diarrhea and protein loss
There is a disease called protein losing enteropathy.
In fact it's several diseases, but in each case, diarrhea is associated with losing protein.
Sometimes with hepatic effects (liver) sometimes not. This because the liver is downsteam of our intestines, receiving their products of digestion.
In a previous post, we discovered that those presenting with COVID-19 usually have (among other findings at the laboratory) low serum albumin. Albumin of course, being a protein.
One place they are losing it from is from the gut.
Not everyone has involvement of the gut, but for those that do, this becomes more important.
Here is some pertinent literature:
COVID-19 and the Digestive System.
Involvement of digestive system in COVID-19 - manifestations, pathology, management & challenges.
Protein Losing Enteropathy - diagnosis and management.
Mount Sinai COVID-19 autopsy experience.
Autopsy Findings in 32 Patients with COVID-19 - a single institution experience.
Summary:
- I learned about protein losing enteropathy (PTE) especially when caring for newborns in the PICU Nursery at Children's Hospital in DC. They would catch a virus, often a rotavirus, then it was off to the races trying to catch up with their fecal protein losses. If we caught up, things went well. If not, well ...
- The last two are from the Pathologists. Always try to arrive as late as possible to your consultation with a Pathologist. The report from Mount Sinai was sent to me by Janet Shapiro, MD. This in response to my questions about GI tract involvement. She is Director of the Medical ICU's at Mount Sinai Hospital in New York, and their affiliated hospitals. She had COVID-19, recovered and is back at work, on a positive note. We've become friends and communicate pretty often when indicated. The point here is that Pathologists have confirmed the gut as a portal of entry for this virus (as with many other viruses). Sometimes the gut is found to have been damaged, sometimes not. But the intestine (duodenum, small bowel, colon) is involved much more often than was initially thought in March/ April. And doing what the gut does (absorbing nutrients) not only supplies energy to the body eventually, it requires energy to get its work done. So the pathologists, at a microscopic level, are finding that the cells that line the intestine are pooped out (pun intended). Cells are seen to be diffusely in a low energy state (don't worry about the details of how they define that. Or if you like, look at the microscopic images at the end of the article from Janet at Mount Sinai, and form your own impression).
- That protein loss becomes a target in those who are ill, but who don't yet need a Path Consult. Just as it was an impotant target for the rug rats I cared for at Children's.
- Another related point. Not only did the Pathologists see with their microscopes, viral particles in the GI cells, but in addition swabs from inside of the intestine (same principle as nasal swabs for diagnosis), were invariably positive in these, ... clients.
- Further comment and explanation possible but not necessary.
-------
Into practice:
- First of all, if your physicians in New York back home already covered this, go with their recommendations. If not, read on.
- Stay well hydrated. When we had to order preparations before surgery for a procedure on the intestine (usually the colon), washing out was always accompanied by lots of liquids from above as well as the enemas from below. I'll save you the enemas as a recommendation. (Here, take a deep breath). If one drinks in a hurry, 3 to 4 liters of water or sports drinks, it will invariably prompt trips to the bathroom for watery diarrhea (as well as peeing more). The point: Make sure you are drinking more than usual. If you exaggerate with tap water, it will drop your serum sodium. So use other liquids as well. Can also ask about available salt-containing choices at the source mentioned below.
- VERY IMPORTANT. Even if the goal is not muscle building, now is a very good time to increase oral protein intake. Just like with the rug rats with their rotavirus infections in Pediatrics. Doing so gets better outcomes. Even after the diarrhea stops, since there is always some catching up to be done.
- I recommend a protein source like Pete used to take in Hawaii. He can be the Team Leader for this effort.
- I recommend taking two scoops to start with, twice a day, then working up to 2 scoops, 3 times a day for the next 2 weeks. A dose of "2 scoops" should supply about 35 to 30 grams of protein. So adjust "scoops" according to the product obtained. You'll know when you're getting into range when you notice your fingernails are gowing more rapidly.
- Do not worry that you'll also be feeding the viruses. They don't like the stuff and never touch it, not even with their spike proteins to get a little taste. It gives them gas.
- I suggest contacting some friends of mine on Bermuda: Kathy Lipp and her husband Gerhard. They carry an ISOPURE product that should do the trick. When you speak with them, ask for a product that is Whey ISOLATE, and not just whey. For those of us who are genetically prone to some degree of lactose intolerance, the ISOLATE form bypasses most of that problem.
- Anticipate nevertheless that this may increase flatulaence just a bit. Of course in the current setting, you can apply this as an appropriate test for anosmia. Also making it more socially defensible: a medical emergency.
- All three can take some. That way the small amount of added flatulence will become habitual and less noticed.
Here are the coordinates for Kathy and Gerhard at Better Health Ltd. If I recall, their store is in the central part of the island, near the Church and the Bermuda Historical Society. Perhaps on the other side of Hamilton Harbor from where you are. (That reminds me, I don't know where you are confined, I mean, ... staying).
So here is their contact information.
I'm sure you can arrange with them, a method of getting this delivered to you.
When you speak with them remember:
- whey protein ISOLATE
- talk over flavors with Pete. Banana, vanilla, chocolate, strawberry are commonly available. I can't stand any of them but chocolate, but do nevertheless consume what I have in stock.
- perhaps a few bottles of a sprots drink that has salts as well as water. (These tend to be disfavored in Medicine, as of no use, unless situations are unusual. Drink plain water, and the body will adjust the needed salts is a very solid Medical principle. Nothwithstanding that truth, this may be an unusual situation). Could mix the protein with this to get both effects. Don't have to.
- 2 or 3 shaker bottles to mix the stuff, or a fancy electrified one.
- It will all be coming in from "outside," so appropraite precautions for 24 hours before use by the two "tested negatives" in the group. For that 3rd person who is now a pariah, he can just have at it when it arrives.
Better Health Ltd.
https://betterhealth.bm/about-us/
SHOP HOURS
Monday - Friday 9 am - 5 pm
Saturday 11 am - 2 pm
Sunday Closed
Better Health Ltd.
Victoria Place, Lower Level,
Hamilton , Bermuda
441.292.4505
And very best of wishes to you three from Christiane here in Stavelot.
Carry on. I agree that Bermuda still has advantages over "back home" given rising numbers on the mainland. As long as clinical status stays stable and leans towards improvement, I agree.
First sign of persistent degradation of that status,... get those jet engines humming.
While flying you back, but not going to a hospital once arrived, may seem like Citi participating in a nice vacation more than emergency medical transport, perhaps home would be just as effective if a few bits of added equipment are put in place. Acceptable?
Symptomatic Management of COVID-19 diarrhea
Recommendations here are based on:
- Review of literature on COVID-19 associated diarrhea (presented here in references)
- Basic principles of management of infectious diarrhea
The principles to apply:
- this illness spreads by the fecal-oral route. The virus was on a surface, was picked up with hands, food, utensils, plasticware, and carried to the mouth and digestive tract. This is quite identical to transmission of many bacterial "gastro" infections.
- the person with the diarrhea now, must accept that shedding of the virus and carrying it to surfaces in bathrooms, dinnerware, clothing, linen, via hands is possible or probable for more than a month.
- while slowing the diarrhea (i.e., reducing frequency and amounts passed) would seem desirable for comfort, medications to this purpose (Lo-Motil, Codeine, others) with the goal of slowing transit through the GI tract are probably to be avoided. Giving the virus more time in the small intestine for example, provides more time for invasiveness across the intestinal lining and is counterproductive.
- the best barrier to invasion of the viral particles is a healthy gut "microbiome," the trillions of 'friendly' bacteria with which the intestine is colonized. These should be increased in number and supported.
- while it has yet to reach common usage, one additional method of "support" can be the application of photobiomodulation (PBM) to the abdomen, using read and near-infrared light.
The practice:
- A dedicated set of utensils, dinnerware, clothing, etc. Developing a conscious awareness of touching little or nothing that will be transferred to other spaces and people. Though not focused here on respiratory risks from the virus, droplets and aerosols from speaking, sneezing, coughing, etc., do settle out onto surfaces. Before they have a chance to do that, frequent air exchanges (hourly), creating drafts with several windows opened, can help.
- All items routinely contacted are either washed frequently, surfaces sprayed with a 1.5 to 2% solution of bleach, or placed in a space or box for sterilization/ decomtamination using UV-C light. This is effective, works fast (15 minutes) and is safe if properly applied. It is the perfect thing for keys, smartphones, masks, walkie-talkies, reading glasses and other items that can not be washed or sprayed with a disinfectant. These UV-C devices are inexpensive. They work by either direct destruction of the virus, or creation of locally increased ozone concentrations that are also viro-toxic. During their application persons should leave the area.
- While not using medications that "relieve" diarrhea, maintaining adequate hydration is mentioned as important. Typically small more frequent meals are advised. Each individual will learn what works best. The duration of the diarrhea is thankfully usually less than in some other GI infections. The concern remains that even after the diarrhea terminated, fecal shedding in normal stools is probable as suggested above.
- Probiotics would seem a logical addition to the treatment plan. While the studies on which strains of "good" bacteria to chose in the case of COVID-19 are still lacking, those used for other infections with "harmful" bacteria can be relied upon. (see images below).
- In the category of "can't hurt," and will probably help, is application of red (660 nm) and near-infrared (830-850nm) light across the abdomen. This in support of the energetics at play. The virus is robbing energy from gut cells and bacteria. The light can restore that. Applied at a distance of 6 to 8" away, for a 10 minute session once or twice a day initially, then daily to every other day, is suggested. This light can also be placed in a box equipped with UV-C light to sterilize it as needed.
Specific advice on the above pro-biotics:
1. Vitacost Probiotic 15-35 15 Strains - 35 billion CFU† per serving -- 120 Vegetarian Capsules
2. NOW Saccharomyces Boulardii -- 5 billion CFU - 60 Veg Capsules
Trish had ordered and rapidly received some Zinc and Copper for her knee from the same place (VitaCost.com).
A suggestion: somewhere on Bermuda must be a pharmacy that can sell you some pro-biotics and deliver to your hotel. Tell the pharmacist you're looking for: "a pro-biotic with about 35 billion colony forming units (CFU's). Also need some Saccaromyces B., if you have some."
Once you have it in hand, take 2 capsules of the pro-biotic when you get it. Then, 1 capsule of the probiotic twice a day. Take a Sacc.B. once a day as well.
---------
Red light: I'm working on that. I sent one to Trish for her patella, at the Otter Rock address. Should be there soon or mayba already arrived. I'm currently trying to find someone who has one on Bermuda. So I'll get back to you on that.
---------